

Abstract
Introduction:
Despite data supporting the safety and efficacy of treatment for many older adults with AML, <40% of adults aged ≥65 receive any leukemia-directed therapy. The reasons for why the majority of older patients with AML do not receive therapy are unclear. The use of objective fitness measures (e.g. physical function and cognition) has been shown to predict outcomes and may assist with treatment decision-making, but is underutilized. As most patients are initially evaluated in community practices, exploring clinical decision-making and the barriers to performing objective fitness assessments in the community oncology setting is critical to understanding current patterns of care. We conducted a qualitative study: 1) to identify factors that influence treatment decision making from the perspectives of the community oncologists and older patients with AML, and 2) to understand the barriers to performing objective fitness assessments among oncologists. The findings will help to inform the design of a larger study to assess real-life treatment decision-making among community oncologists and patients.
Methods:
We conducted semi-structured interviews with 13 community oncologists (9 states) and 9 patients aged ≥60 with AML at any stage of treatment to elicit potential factors that influence treatment decisions. Patients were recruited from the outpatient clinics in a single institution and oncologists were recruited via email using purposive samples (patients: based on treatment received and stage of treatment; oncologists: based on practice location). Interviews were audio-recorded and transcribed. We utilized directed content analysis and adapted the decision-making model introduced by Zafar et al. to serve as a framework for categorizing the factors at various levels. A codebook was provisionally developed. Using Atlas.ti, two investigators independently coded the initial transcripts and resolved any discrepancies through an iterative process. The coding scheme was subsequently applied to the rest of the transcripts by one coder.
Results:
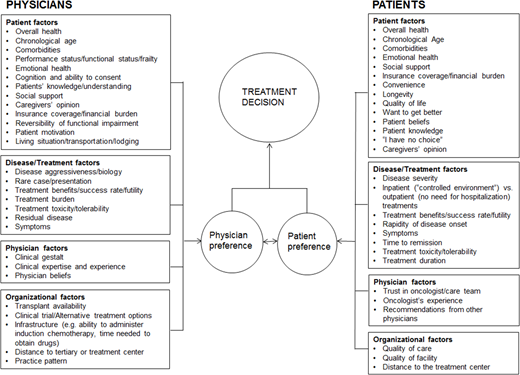
Median age of the oncologists was 37 years (range 34-64); 62% were females, 92% were white, 38% had practiced more than 15 years, and 92% reported seeing <10 older patients with AML annually. Median age of the patients was 70 years (64-80), 33% were females and all were Caucasian. In terms of treatment, 66% received intensive induction therapy, 22% received low-intensity treatment, and 11% received both. Three patients also received allogeneic hematopoietic stem cell transplant. Eighty-nine percent were initially evaluated and 56% were initially treated by a community oncologist. Factors that influenced treatment decision-making are shown in Figure 1. When making treatment decisions, both patients and oncologists considered factors such as patient's overall health, chronological age, comorbidities, insurance coverage, treatment efficacy and tolerability, and distance to treatment center. Nonetheless, there were distinct factors considered by patients (e.g. quality of care and facility, trust in their oncologist/team) and by oncologists (e.g. local practice patterns, availability of transplant/clinical trials, their own clinical expertise and beliefs) when making treatment decisions. The majority of oncologists do not perform an objective assessment of fitness. Most common reasons provided included: 1) Do not add much to routine assessments (N=8), 2) Lack of time, resources, and expertise (N=7), 3) Lack of awareness of the tools or the evidence to support its use (N=4), 4) Specifics are not important (e.g. impairments are clinically apparent and further nuance is not necessarily helpful; N=5), 5) Impairments are usually performed by other team members (N=2), and 6) Do not want to rely on scores (N=2).
Conclusions:
Treatment decision-making for older patients with AML is complex and influenced by many factors at the patient, disease/treatment, physician, and organizational levels. Despite studies supporting the utility of objective fitness assessments, these were not commonly performed in the community due to several barriers. Our framework will be useful to guide a larger study to assess real-life treatment decision-making in the community settings. We also identified several barriers raised by community oncologists that could be targeted to allow incorporation of objective fitness assessments.
Liesveld:Onconova: Other: DSMB; Abbvie: Honoraria. Stock:Jazz Pharmaceuticals: Consultancy. Majhail:Anthem, Inc.: Consultancy; Atara: Honoraria; Incyte: Honoraria. Wildes:Janssen: Research Funding. Klepin:Genentech Inc: Consultancy.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal